If you're researching TMS for treatment-resistant depression, there's a good chance you've already been through multiple antidepressant medications without adequate relief. You may have tried two, three, or more, each time adjusting the dose, waiting weeks for it to take effect, managing the side effects, and eventually concluding it wasn't working. That pattern is more common than most patients realize, and it says more about the limitations of medication as a treatment category than it does about you.
Transcranial magnetic stimulation (TMS) works on a fundamentally different mechanism than antidepressant medications. Rather than changing neurotransmitter levels across the brain, TMS uses magnetic fields to directly stimulate nerve cells in parts of the brain involved in mood regulation.
That distinction matters for treatment-resistant depression (TRD) specifically: a failed medication trial tells you that adjusting brain chemistry systemically wasn't sufficient. It doesn't tell you that direct brain stimulation won't work. They're addressing the problem from different angles.
This article is specifically about TMS as a treatment for depression that hasn't responded to medication or other treatments. It covers why TMS works differently, how the protocols compare (standard, accelerated, and fMRI-guided), what the TRD-specific evidence shows, and what’s involved in every treatment session.
In This Article
If you want a broader comparison of all evidence-based treatment options for TRD—including electroconvulsive therapy (ECT), ketamine, Spravato, psychotherapy, and medication strategies—see our complete guide to treatment-resistant depression treatment options.
Note: Cognitive FX offers fMRI-guided accelerated TMS with approximately 79% remission rates in clinical research. To see if you're a candidate, take a short quiz or call 385-334-6093.
How TMS Works Differently Than Antidepressant Medications
The question many TRD patients have isn't "how does TMS work?" in the abstract. It's "why would this work when medications haven't?" The answer comes down to mechanism. TMS therapy and antidepressant medications treat depression through entirely different pathways.
What Antidepressant Medications Do and Where They Fall Short
SSRIs, SNRIs, tricyclics, MAOIs, and other antidepressant medications work by modifying the availability of neurotransmitters (primarily serotonin, norepinephrine, and dopamine) throughout the brain. The underlying assumption is that depression results from insufficient neurotransmitter activity, and that increasing it will produce relief.
For roughly one-third of people with major depressive disorder, that assumption holds well enough: they achieve remission with their first medication. But a reanalysis of the landmark STAR*D study (the largest real-world antidepressant trial ever conducted, involving over 4,000 depressed patients) found that with each successive medication trial, the odds of response drop significantly.
Among patients whose symptoms persisted after two types of antidepressant medications failed, less than 2% experienced success with a third or fourth medication.
In short, when multiple antidepressant medications fail, the problem is usually more than a neurotransmitter imbalance. Research increasingly points to disrupted neural circuits. Specifically, reduced connectivity between the dorsolateral prefrontal cortex (DLPFC) and deeper mood-regulating structures, such as the subgenual cingulate cortex, is a core driver of TRD. Medications don't directly address that circuit-level dysfunction. TMS does.
How TMS Targets the Brain Differently
TMS uses a magnetic coil placed against the scalp to deliver magnetic pulses that pass through the skull and induce small electrical currents in the underlying nerve cells. Those currents stimulate neurons in the target region, increasing activity in brain circuits that have become underactive.
For depression treatment, the target is the left dorsolateral prefrontal cortex (L-DLPFC), a region of the brain consistently shown to be hypoactive in depressed patients. The DLPFC is involved in executive functioning, attention, motivation, and the regulation of emotional responses. When it's underactive, and when its connections to deeper emotional processing centers (the subgenual cingulate, the amygdala) are weakened, the result is the constellation of depressive symptoms: low motivation, difficulty experiencing pleasure, cognitive fog, emotional numbness, and persistent negative mood.
One way to think about it: People with depression constantly hear “just snap out of it.” The advice is useless, but the underlying concept is real. People who aren't clinically depressed can, in fact, redirect themselves away from negative thinking. They have a functional regulatory switch in the prefrontal cortex that allows them to do that. In TRD, that switch is weakened. TMS strengthens it. The treatment doesn’t directly suppress the overactive emotional centers; instead, it builds up the regulatory circuit that's supposed to keep those centers in check.
What’s Happening at the Cellular Level
At the cellular level, TMS pulses boost blood flow to the target area, increase neurotrophin production (proteins that support neuronal health and growth), stimulate neurotransmitter release, and increase neuronal responsiveness to input. With theta burst stimulation specifically, the pulse pattern mimics a natural brain rhythm that neurons readily entrain to. The brain responds to it the way a muscle responds to a stretch. The result is increased functionality, not disruption. TMS doesn't put anything new into the brain or remove anything from it. It marshals the neural resources talready there and aren't being used effectively.
A related concern patients sometimes raise: if TMS induces neuroplasticity (changes in how the brain is wired), could it change the brain in the wrong direction? The answer is no, and the reason is important. TMS isn't reorganizing a healthy brain into something different—it's organizing a brain that has become disorganized by depression. The disorganization is where the symptoms come from. When you induce plasticity in a disorganized system, it doesn't rearrange randomly. It moves toward its designed baseline. The neuroplasticity TMS produces is restorative, not experimental.
This mechanistic distinction is why medication failure doesn't predict TMS failure. A meta-analysis of repetitive transcranial magnetic stimulation in treatment-resistant populations confirmed that TMS produces clinically significant improvement even in patients who have not responded to multiple antidepressant treatments. A 2022 randomized, double-blind, sham-controlled crossover study found a 63% response rate and 42% remission rate among TRD patients receiving TMS alongside pharmacotherapy. The two interventions target different aspects of the pathology, which is exactly why one can succeed where the other fails.
TMS Protocols Compared: What Matters for TRD Patients
Not all TMS treatment is the same. The term covers several distinct modalities that differ substantially in how they target the brain, how long treatment takes, and how effective they are, particularly in TRD populations.
The two broad categories are standard repetitive TMS (the original 6-week protocol) and accelerated TMS (compressed-schedule protocols that deliver higher doses over days rather than weeks). Within accelerated TMS, the critical variable is whether the protocol includes fMRI-guided targeting, which is the single factor most strongly associated with higher remission rates in TRD.
Standard Repetitive TMS (rTMS): The 6-Week Protocol
Standard repetitive TMS (rTMS) is the original form of the treatment and remains the most widely available. It was first FDA-approved for major depressive disorder in 2008 by the US Food and Drug Administration, and it has been the subject of more than 360 studies, including numerous randomized clinical trials and meta-analyses specifically addressing TRD.
How It Works
Daily treatment sessions, five days a week, for 4–6 weeks (typically 36 sessions total). Each session delivers approximately 3,000 high-frequency magnetic pulses to the left DLPFC over 30–40 minutes. The magnetic coil is positioned based on scalp measurements, a method that estimates where the DLPFC is by measuring distances from the patient's nose, ears, and the top of the head. The clinician first determines the patient's resting motor threshold (the minimum stimulation intensity needed to produce a visible muscle twitch in the hand), then sets the treatment intensity relative to that threshold (typically 110–120%).
TRD-Specific Evidence
Standard rTMS achieves remission in approximately 30–36% of treatment-resistant patients, with response rates of approximately 50%. A systematic review and meta-analysis published in Neuropsychopharmacology confirmed a statistically significant advantage over sham stimulation in TRD populations, though the effect sizes were moderate.
When combined with psychotherapy, specifically cognitive behavioral therapy (CBT), outcomes improve substantially. Combined, TMS and CBT produce approximately 66% response rates and 55% remission rates, versus ~50% response and ~30% remission for rTMS alone. That's a meaningful difference, and it suggests that pairing brain stimulation with structured psychotherapy addresses the problem from multiple angles simultaneously.
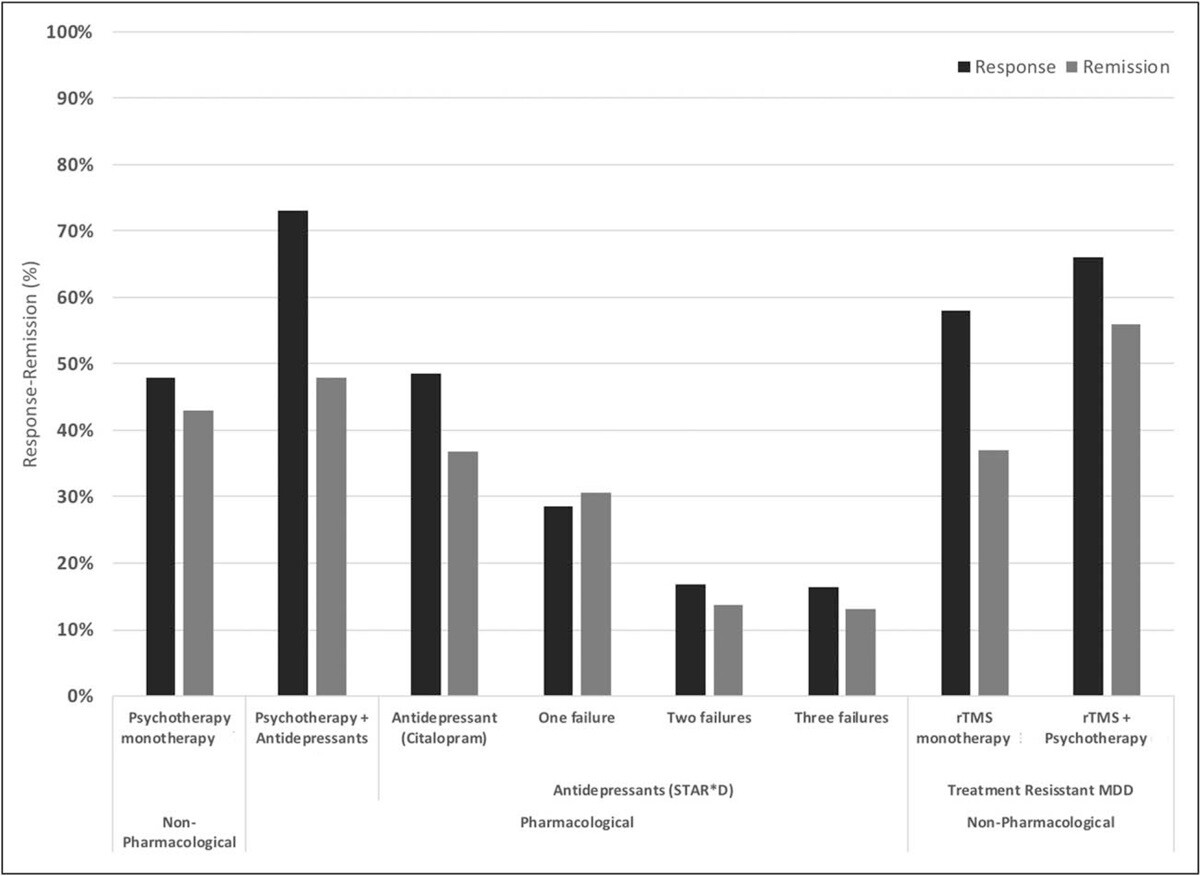
Response and remission rates of various monotherapeutic and combinatory antidepressant treatments based on the largest studies and datasets available. [Source]
Durability
Among responders, approximately 50% maintain their improvement at one year with continuation treatment (tapering from weekly to monthly sessions alongside optimized medications). Without any follow-up, relapse rates reach approximately 80%. The encouraging finding: when symptoms do return, reintroducing TMS produces an 84.2% success rate, suggesting the brain retains some of the circuit changes from the initial course.
Insurance
Standard rTMS is the only TMS protocol routinely covered by insurance. Most major insurers cover it after documented failure of 2–4 antidepressant medications. For details on coverage requirements and out-of-pocket costs, see our guide on whether insurance covers TMS therapy.
The Practical Limitation
Six weeks of daily clinic visits is a genuine barrier for many TRD patients. Depression itself often makes it difficult to maintain daily commitments, and the time commitment can conflict with work, caregiving, and other healthcare appointments. For more on how long TMS takes to work (and what the experience involves), and for a balanced look at the pros and cons of TMS therapy, we've covered both topics separately.
Targeting Limitation
Scalp-landmark targeting can be imprecise. Because head size, shape, and individual brain organization vary substantially between people, the "5-7 rule" used for coil placement can miss the optimal DLPFC site by up to 2 centimeters. For a brain region where stimulation accuracy directly affects outcomes, that margin of error is significant. It is one of the primary predictors of why standard rTMS doesn't work for some patients.
Accelerated TMS: Compressed Schedule, Higher Dose, Precision Targeting
Accelerated TMS compresses treatment into days rather than weeks, typically delivering multiple sessions per day over the course of one week or less. Most accelerated protocols also use intermittent theta burst stimulation (iTBS), an FDA-approved pulse delivery method that mimics the brain's natural theta rhythm. Each iTBS session takes approximately 10 minutes rather than 30–40 minutes, making multiple daily sessions feasible. For a comparison, see our detailed article on the differences between rTMS and iTBS.
The compressed format solves one of standard rTMS's biggest practical problems: six weeks of daily clinic visits is a genuine barrier for patients whose depression makes it difficult to sustain daily commitments.
For more on accelerated TMS, including how tofind accelerated TMS near you, see our accelerated TMS overview.
The Variable That Matters Most: fMRI-Guided Targeting
The compressed schedule and iTBS pulse delivery are meaningful advances, but neither explains the largest difference in TRD outcomes. That comes from how the treatment is targeted.
Most accelerated TMS protocols still position the magnetic coil using the same scalp-landmark method as standard rTMS. That means the 2-centimeter targeting limitation described above still applies. The protocol that has produced the highest remission rates to date, the Stanford Accelerated Intelligent Neuromodulation Therapy (SAINT™), adds a third layer: personalized fMRI-based targeting.
The original SAINT clinical trials produced results that were markedly different from standard TMS outcomes, and the protocol has since been replicated and studied at multiple institutions. The protocol combines the accelerated schedule and iTBS with functional MRI imaging that maps each patient's individual brain activity before treatment begins. The imaging identifies the specific spot in the left DLPFC that shows the weakest connectivity to deeper mood-regulating networks—the exact location where stimulation is most likely to restore normal circuit function. An FDA-approved neuronavigation system then guides the magnetic coil to that precise spot, with accuracy within 1–2 millimeters.
The SAINT protocol delivers 10 sessions per day for 5 days, 50 sessions total, totaling approximately 90,000 pulses. Standard rTMS delivers 18,000–20,000 pulses over 6–9 weeks. The concentrated dosing, combined with precision targeting, creates more rapid and more robust changes in neural circuit activity.
Note: SAINT™ is a trademark of Stanford University, exclusively licensed to Magnus Medical. Cognitive FX is not affiliated with, endorsed by, or licensed to provide SAINT, and does not use Magnus Medical equipment. We offer fMRI-guided intermittent theta burst TMS, with target locations determined by fMRI and our prescribing physician. We reference SAINT here only to compare treatment options.
TRD-Specific Evidence
The results from the SAINT clinical trials are the strongest published to date for any TMS protocol in treatment-resistant depression. In the double-blind, sham-controlled trial, approximately 85% of participants showed significant improvement (response), and approximately 78% achieved full remission within five days. All participants had treatment-resistant depression and had failed at least two prior antidepressant treatments. At four-week follow-up, approximately 60% maintained remission.
Clinical research on fMRI-guided TMS more broadly has demonstrated approximately 79% remission rates.
For context: standard rTMS achieves approximately 30–36% remission in TRD populations. ECT achieves approximately 48% remission. SSRIs and other antidepressant medications achieve approximately 33% remission on first-line treatment, declining with each subsequent trial. The fMRI-guided accelerated protocol roughly doubles the remission rate of any other established modality.
A separate finding from the open-label phase of the Stanford trials is particularly notable for patients experiencing severe depressive symptoms: all 21 participants who reported suicidal ideation before treatment reported none after completion.
How Long Do Results Last?
Durability has been one of the important open questions about the SAINT protocol. A 2025 study provides the most complete answer to date. Without any maintenance treatment, 47% of patients who achieved remission maintained it at three months, a median duration of approximately 3.5 months comparable to ECT and standard TMS without follow-up care.
With personalized maintenance, the picture changes substantially. A personalized continuation therapy study found that 86% of participants maintained remission over 12 months when early warning signs of relapse triggered retreatment. Most retreatment courses required only 1–2 days rather than a full repeat of the five-day protocol. For more on how long TMS results last and what maintenance looks like, see our dedicated article.
For a broader comparison of TMS success rates across protocols, including standard rTMS, deep TMS, and accelerated approaches, we've compiled the data in a separate comparison piece.
Can Accelerated fMRI TMS Work If Standard TMS Already Failed?
This is one of the most common questions from TRD patients who have already tried rTMS without success, and one that most healthcare providers don't address clearly enough.
The short answer: yes, and the evidence supports it. The Stanford SAINT trials specifically enrolled patients who had failed other TMS approaches, and the results (78% remission) still held for that population. The explanation for why fMRI-guided TMS can succeed where standard rTMS failed comes back to targeting precision.
When standard rTMS doesn't produce adequate results, the most likely reason isn't that "TMS doesn't work for this patient." It's that the magnetic coil wasn't placed over the right spot. The DLPFC isn't a single point—it's a region, and the optimal stimulation site within it varies between individuals. Scalp-landmark positioning assumes that the relationship between external skull features and internal brain anatomy is consistent across patients. It isn't. Studies using neuroimaging have demonstrated that the conventional "5-7 rule" for coil placement sometimes misses the intended target entirely.
With fMRI-guided targeting, the optimal site is identified from the patient's own brain activity rather than estimated from external measurements. Neuronavigation then ensures the coil returns to that exact spot every session. For patients who were previously non-responders to standard rTMS, this precision can make the difference between an effective treatment and an ineffective one.
If you've been through rTMS treatment previously without adequate relief, it's worth having a conversation about what targeting method was used and whether fMRI-guided neuromodulation might produce a different result.
For more on this topic, see our article: What if TMS doesn't work?
What a Week of Accelerated TMS Treatment Looks Like
The clinical data on TMS are well documented, but most sources don't describe what the experience actually involves on a practical level. If you're considering a five-day accelerated protocol, here's what to expect.
Before Treatment Starts
The process begins with a screening consultation. The clinician reviews your mental health history, current medications, and any contraindications (history of seizures or epilepsy, metallic implants near the head, bipolar disorder, or other conditions that might affect eligibility). For protocols that include fMRI-guided targeting, you'll undergo a functional MRI scan before treatment begins. This is a non-invasive brain scan lasting approximately 15–20 minutes, during which the imaging maps your brain's resting-state activity and identifies the personalized stimulation target.
You'll also discuss expectations: when improvement is likely to start, and what the TMS dip is. Some patients experience a temporary worsening of mood in the first one to three days before improvement begins. This can feel contradictory if you've been told TMS doesn't cause harm, and technically, it doesn't. What's happening is that the plasticity process temporarily loosens the existing (dysfunctional) neural patterns before they consolidate into better-organized ones. Think of it like physical therapy after an injury: the first sessions can make you more sore before mobility improves. The dip, when it occurs, is brief, self-resolving, and does not predict a negative outcome. Patients who experience it still go on to achieve remission at the same rates.
A Typical Treatment Day
For the accelerated iTBS protocol, a treatment day involves 10 TMS sessions, each lasting approximately 10 minutes. Sessions are spaced roughly 50 minutes apart to allow the brain time to consolidate the effects of stimulation between rounds. The total time at the clinic is most of the day.
During each session, you sit in a reclining chair while the magnetic coil is positioned over the identified target site. The coil delivers pulses in the iTBS pattern, brief bursts that produce a clicking or tapping sensation against your scalp.
One thing worth knowing: the scalp sensation is more intense than the brain effect. The magnetic pulses activate cranial nerves, particularly the trigeminal nerve, which carries pain signals from your sinuses and teeth, so the surface experience can feel jarring. Jaw clenching and localized headache are common, especially in the first sessions. Patients sometimes assume that if it feels harsh on the outside, something harsh must be happening to their brain. The opposite is true. The effect on the underlying neural tissue is mild and stimulatory—the brain responds to the theta burst rhythm readily, almost naturally. The discomfort is a scalp and muscle phenomenon, not a brain one, and it typically diminishes as you acclimate over the first few sessions. For a detailed account of what TMS feels like, see our separate article.
Between sessions, you rest, eat, walk around, or read. The treatment is fully outpatient. No anesthesia, no sedation, no fasting required. You remain alert throughout.
In protocols that incorporate cognitive behavioral therapy (CBT) alongside TMS, which evidence suggests improves remission rates by approximately 19% compared to TMS alone, therapy sessions are woven into the daily schedule between stimulation sessions. The goal is to pair the neurological changes produced by TMS with the cognitive restructuring that CBT provides, reinforcing both the biological and psychological aspects of recovery.
After the Five Days
The majority of patients who respond to fMRI-guided accelerated TMS begin noticing meaningful shifts in mood, motivation, or cognitive clarity within the first three days of treatment. Some experience the full effect by the end of the treatment week; others see continued improvement over the two to four weeks following treatment.
Follow-up assessment typically occurs two to four weeks after the treatment course. This is where clinicians evaluate the degree of response and plan ongoing care. For patients who achieve remission, the maintenance question becomes relevant: if symptoms begin to return, retreatment with the accelerated protocol typically requires 1–2 days rather than repeating the full five-day course.
TMS treatment is not a replacement for ongoing mental health care. Continued psychotherapy, medication optimization, and lifestyle factors (exercise, sleep, social support) all contribute to sustained improvement. The role of TMS is to address the neurological circuit dysfunction that medications alone can’t reach. It creates a window of improved brain function within which other evidence-based interventions can work more effectively.
Side Effects and Safety
If you've spent years on antidepressant medications, you're likely familiar with systemic side effects: weight gain, sexual dysfunction, emotional blunting, insomnia, and difficulty tapering off. TMS has a fundamentally different side effect profile because it works locally, not systemically.
Before covering the specifics, one point that comes up frequently in patient consultations and is worth addressing directly: online forums and social media groups include accounts from people who report that TMS "ruined their life" or caused lasting harm. These reports are understandably alarming. Here is what the clinical evidence and neurophysiology say about them.
Every TMS device approved by the FDA went through validation studies that required comprehensive reporting of all adverse events. None of those studies documented the kind of catastrophic outcomes described in those online accounts. More fundamentally, there is no known physiological mechanism by which TMS damages neurons. The pulses boost blood flow, boost the production of neurotrophins and neurotransmitters, and make cells more responsive. Even if the coil is placed over a suboptimal target, the effect is to improve the functionality of whatever region is stimulated; it just might not address the patient's specific symptoms.
The worst realistic outcome of TMS is that it doesn't produce a meaningful benefit. That's a disappointing outcome, but it's not a harmful one. We can't account for every individual subjective report, but the clinical and physiological evidence consistently supports this conclusion.
Common Side Effects of TMS
The most frequently reported effects are mild and localized:
- Scalp discomfort or tenderness at the stimulation site, typically diminishing after the first few sessions
- Headaches are usually mild and responsive to over-the-counter analgesics
- Lightheadedness or facial tingling during treatment, brief and self-resolving
TMS does not produce systemic side effects. There is no weight gain, no sexual dysfunction, no emotional blunting, and no withdrawal syndrome. You remain fully alert during treatment and can drive yourself to and from the clinic. This side effect profile is one of the primary reasons clinicians consider TMS for patients who have experienced significant medication-related adverse effects.
For a detailed review of the side effects of TMS, including benefits versus risks, see our full article. And for a broader look at TMS safety, see: Is TMS safe?
Serious Risks
The most significant risk associated with TMS is seizure. The incidence is extremely rare: less than 0.01% per session, or fewer than 1 in 10,000 treatment sessions. Screening protocols exclude patients with seizure disorders or epilepsy, and treatment parameters are calibrated to the individual's motor threshold to stay well within established safety limits. TMS does not involve electrical current passing through the brain (unlike ECT); the magnetic pulses induce localized currents in superficial cortical neurons only.
Patients with metallic implants near the treatment site (cochlear implants, aneurysm clips, deep brain stimulators, or metal plates) are generally excluded from TMS because the magnetic field can interact with these devices. Standard dental fillings and braces are not a concern.
For more information on whether TMS can worsen existing symptoms, see our articles on whether TMS can make depression worse and whether TMS can make anxiety worse.
Can You Stay on Antidepressant Medications During TMS?
Yes. Most patients continue their current antidepressant medications during TMS treatment. Some medications that substantially lower the seizure threshold may need to be adjusted, but this is handled on a case-by-case basis with the prescribing clinician. For a detailed discussion of combining antidepressant medication with TMS, see our dedicated article.
Who Is a Good Candidate for TMS (and Who Should Avoid It)
Good Candidates for TMS
The evidence base for TMS is strongest in patients with treatment-resistant depression, specifically those who have tried at least two antidepressant medications at adequate doses for adequate duration without sufficient improvement. That is the clinical definition of TRD, and it is typically the threshold insurers use for standard rTMS coverage as well.
Beyond the TRD criteria, TMS is a strong option for patients who:
- Have moderate to severe major depressive disorder that significantly affects daily functioning
- Want to avoid or reduce the systemic side effects of additional medication trials
- Are between 18 and 65 years old (the studied population for most protocols)
- Can commit to the treatment schedule: one week for accelerated protocols, or six weeks for standard rTMS
- Experience comorbid anxiety alongside depression. Research on TMS for anxiety shows benefit, and several studies have demonstrated improvement in anxious depressive symptoms specifically. For more on this, see our article on anxious depression treatment.
To evaluate whether you may be a good candidate for the accelerated fMRI-guided protocol specifically, see: Is SAINT TMS right for me?
Who Should Not Receive TMS
TMS has relatively few absolute contraindications, but the following groups should not receive treatment:
- Patients with a history of seizures or epilepsy
- Patients with metallic objects in or near the head (cochlear implants, aneurysm clips, deep brain stimulators, internal pulse generators, shrapnel). Braces and dental fillings are acceptable.
- Patients who are currently in acute suicidal crisis and need immediate crisis-level care.
- TMS is an effective treatment for depression and has demonstrated reductions in suicidal ideation, but it is not an emergency intervention.
- Patients taking certain medications that significantly lower the seizure threshold (discuss specific medications with your clinician).
What If You've Already Tried Standard TMS?
As discussed above, previous non-response to standard rTMS does not rule out response to fMRI-guided accelerated TMS. The targeting precision of the fMRI-guided approach addresses the most common reason standard TMS fails: imprecise coil placement. If you've been through rTMS without adequate results, the protocol used for targeting is a critical detail to discuss with any provider you're evaluating.
Cost, Insurance, and Practical Considerations
What Does TMS Cost?
The cost of TMS treatment varies significantly based on the protocol, geographic location, and provider:
- Standard rTMS (6-week protocol): $6,000–$15,000 for 36–40 sessions. This is the protocol most likely to be covered by insurance.
- Accelerated TMS (1-week protocols): $6,000–$15,000 without fMRI targeting. Rarely covered by insurance, as accelerated protocols are generally considered off-label.
- fMRI-guided accelerated TMS: $7,000–$36,000 depending on the provider. Medicare began covering the SAINT protocol at $19,703 in July 2025. Private insurance does not currently cover accelerated TMS protocols.
For more detailed cost breakdowns, see our articles: TMS treatment costs and SAINT treatment cost.
Insurance and Coverage
Standard rTMS is covered by most major insurers for patients who meet TRD criteria, typically documented failure of 2–4 antidepressant medications at adequate dose and duration. Coverage determination usually involves prior authorization, and some insurers require evidence of a specific number of failed medication classes.
Accelerated iTBS protocols are typically self-pay. Some clinics, including Cognitive FX, offer pricing significantly below the licensed SAINT product.
Further reading: TMS Insurance Coverage Requirements
Practical Considerations
Time away from work and obligations: The practical difference between one week (accelerated) and six weeks (standard) is substantial for most patients. The accelerated format allows many TRD patients to travel to a specialized clinic, complete treatment in a single week, and return home rather than restructuring six weeks of daily life around clinic visits.
Travel: Fewer than 20 clinics in the US currently offer the complete fMRI-guided accelerated protocol with personalized brain imaging and neuronavigation. For many patients, treatment involves traveling to one of these locations. This is a one-time trip rather than six weeks of local daily visits.
Combining with ongoing care: TMS is not a standalone treatment. It addresses the neurological component of treatment-resistant depression. Ongoing psychotherapy, medication management, and attention to sleep, exercise, and social support all contribute to sustained improvement. The fast-acting relief that TMS provides creates a neurological foundation that other evidence-based therapies can build on. For patients who have also struggled with talk therapy, we've written separately about what to do when therapy isn't working for depression.
Receiving fMRI-Guided Accelerated TMS at Cognitive FX
Standard rTMS achieves remission in roughly 30–36% of TRD patients. That's a meaningful result, but it leaves the majority without adequate relief. Two factors largely explain the gap: imprecise targeting (coil placement based on scalp landmarks can miss the optimal site by up to 2cm) and a 6-week protocol that makes adherence difficult and spreads the neurological stimulus over a long time frame.
Cognitive FX's TMS program addresses both. Treatment begins with an fMRI scan that maps each patient's individual brain activity, identifying the precise location of the DLPFC before any stimulation takes place. An FDA-approved neuronavigation system then guides the magnetic coil to that exact spot for every session, ensuring consistent targeting accuracy within 1–2 millimeters.
The protocol delivers 50 sessions over five days using FDA-approved intermittent theta burst stimulation, totaling approximately 90,000 pulses equivalent in dosage to the Stanford SAINT protocol. Cognitive behavioral therapy is incorporated alongside TMS sessions, which research indicates improves response rates by approximately 8% and remission rates by approximately 19% compared to TMS alone.
The key distinction from the licensed Magnus SAINT™ product: Cognitive FX uses in-house fMRI analysis by a neuroscientist and physician, drawing on 25+ years of clinical fMRI experience from treating brain injury patients. Magnus SAINT™ uses FDA-approved proprietary targeting software. The protocols are otherwise equivalent in dosage, equipment, and schedule. Cognitive FX's program is an off-label equivalent, not the licensed Magnus SAINT™ product. (SAINT™ is a trademark of The Board of Trustees of the Leland Stanford Junior University.)
Clinical research on fMRI-guided TMS has demonstrated approximately 79% remission rates. Cost is $7,000–$12,000, compared to $30,000 or more for the licensed Magnus SAINT™ product. Insurance does not currently cover accelerated TMS; only the standard 6-week rTMS protocol is covered by most major insurers for patients who meet TRD criteria.
Cognitive FX does not treat patients under 18 or over 65 for TMS. Patients with a history of seizures, metallic implants near the treatment site, or who are currently actively suicidal and in need of crisis care are also excluded from the TMS program.
For a side-by-side comparison of the two protocols:
For more on SAINT™ TMS locations and availability across the US, see our article on SAINT TMS locations. We've also covered the full range of options if you want a broader look at alternative treatments for depression beyond TMS.
If you've been through multiple antidepressant medications without lasting relief, fMRI-guided TMS targets the problem from a different angle. You can take a short quiz to evaluate whether you're a likely candidate, schedule a consultation, or call 385-334-6093 to speak with someone directly.
Cited Research
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and Longer-Term Outcomes in Depressed Outpatients Requiring One or Several Treatment Steps: A STAR*D Report. American Journal of Psychiatry. 2006;163(11):1905-1917.
- Cole EJ, Phillips AL, Bentzley BS, et al. Stanford Neuromodulation Therapy (SNT): A Double-Blind Randomized Controlled Trial. American Journal of Psychiatry. 2022;179(2):132-141.
- George MS, Lisanby SH, Avery D, et al. Daily Left Prefrontal Transcranial Magnetic Stimulation Therapy for Major Depressive Disorder. Arch Gen Psychiatry. 2010;67(5):507-516.
- Blumberger DM, Vila-Rodriguez F, Thorpe KE, et al. Effectiveness of theta burst versus high-frequency repetitive transcranial magnetic stimulation in patients with depression (THREE-D). The Lancet. 2018;391(10131):1683-1692.
- Berlim MT, Van den Eynde F, Daskalakis ZJ. Clinically meaningful efficacy and acceptability of low-frequency repetitive transcranial magnetic stimulation (rTMS) for treating primary major depression: a meta-analysis. Neuropsychopharmacology. 2013;38(4):543-551.
- Akpinar K, Oğuzhanoğlu NK, Uğurlu TT. Efficacy of transcranial magnetic stimulation in treatment-resistant depression: a randomized controlled study. Turkish Journal of Medical Sciences. 2022;52(3):752-765.
- Apostol M, et al. Efficacy of 5×5 accelerated versus conventional repetitive transcranial magnetic stimulation (rTMS) for treatment-resistant depression. Journal of Affective Disorders. 2026.
- Geoly AD, Kratter IH, et al. Durability of clinical benefit with Stanford Neuromodulation Therapy (SNT) in treatment-resistant depression. Brain Stimulation. 2025.
- Magnus Neuromodulation System with Stanford Accelerated Intelligent Neuromodulation Therapy (SAINT) as a Personalized Continuation Therapy for Depression: An Open-Label Pilot Trial. Brain Stimulation. 2025.









