Published peer-reviewed research shows that Cognitive FX treatment leads to meaningful symptom reduction in post-concussion symptoms for 77% of study participants. Cognitive FX is the only PCS clinic with third-party validated treatment outcomes.
Post-Concussion Syndrome in Children: Parent's Complete Guide
39:36
When your child's concussion symptoms refuse to go away, every parent faces the same terrifying question: What's happening to my child's brain, and why isn't anyone able to help?
If weeks have passed since your child's head injury and they're still complaining of headaches, struggling in school, or just not acting like themselves, you're not imagining things. And despite what some doctors may have told you, this isn't something your child simply needs to "push through."
Your child may have post-concussion syndrome, a condition that affects between 10% and 30% of children following a concussion. The good news? With proper diagnosis and evidence-based treatment, most children with persistent symptoms can make significant improvements and return to their normal lives.
This guide will walk you through everything you need to know: how to recognize post-concussion syndrome in your child, what the latest research says about recovery, and what treatment options actually work.
The Problem: Why Your Child's Concussion Symptoms Won't Go Away
A concussion is a mild traumatic brain injury caused by a bump, blow, or jolt to the head. In children, the most common causes are falls, sports injuries, motor vehicle accidents, and playground collisions. According to the CDC, emergency departments treat approximately 700,000 children annually for traumatic brain injuries, with falls and sports being the leading causes.
Most children recover from a concussion within two to four weeks. But for a significant percentage, symptoms persist well beyond that window. When concussion symptoms last longer than four weeks in children (or three months using older diagnostic criteria), clinicians diagnose post-concussion syndrome.
What actually happens in a child's brain during PCS?
Post-concussion syndrome isn't about structural brain damage that shows up on CT scans or standard MRIs. In fact, most imaging comes back "normal" in children with PCS, which can be incredibly frustrating for parents searching for answers.
The real problem lies in how the brain functions after injury. Research has identified several key mechanisms:
Neurovascular coupling dysfunction: This is the relationship between neurons (brain cells) and the blood vessels that supply them with oxygen and nutrients. After a concussion, this communication system can become disrupted. Affected brain regions don't receive the right amount of oxygen at the right time, causing them to work inefficiently during tasks like reading, concentrating, or processing information.
Autonomic nervous system dysregulation: The autonomic nervous system controls automatic functions like heart rate, blood pressure, and body temperature. Concussions can disrupt this system, leading to symptoms like exercise intolerance, dizziness upon standing, and temperature sensitivity.
Vestibular and vision system dysfunction: The systems that control balance, spatial awareness, and eye movement are particularly vulnerable to concussion. Research published in the Journal of Sport and Health Science (2025) found that 62% of adolescents with persistent post-concussion symptoms have diagnosable vision disorders, many of which go undetected without specialized testing. [DOI: 10.1016/j.jshs.2025.101058]
Cervical spine involvement: The neck often sustains injury during the same forces that cause a concussion. Neck dysfunction can contribute to headaches, dizziness, and other symptoms that overlap with PCS.
Understanding these mechanisms is crucial because it explains why "just rest" often fails as a treatment strategy and why many children need targeted, multidisciplinary care to recover.
\n Note: This assessment provides general guidance only and is not a substitute for professional medical or educational advice. Formal accommodation decisions should be made in consultation with your child's healthcare providers and school officials.\n
The Agitation: What Parents Don't Know Is Costing Their Children Precious Time
Here's the hard truth that keeps pediatric concussion specialists up at night: most children with post-concussion syndrome are either undiagnosed, misdiagnosed, or given outdated treatment advice that can actually prolong their symptoms.
Many parents hear some version of these frustrating phrases:
"Just give it more time."
"Keep them in a dark room until they feel better."
"It's probably just anxiety."
"The scans are normal, so there's nothing wrong."
Meanwhile, their child continues to suffer, falls further behind in school, and watches friends move on without them.
The 2022 Amsterdam Consensus Statement, the international gold standard for concussion management, fundamentally changed what we know about pediatric concussion recovery. Yet many healthcare providers haven't caught up to the evidence. According to this consensus, the old "cocoon" approach of keeping children in dark rooms with no activity is not only unnecessary but may actually slow recovery.
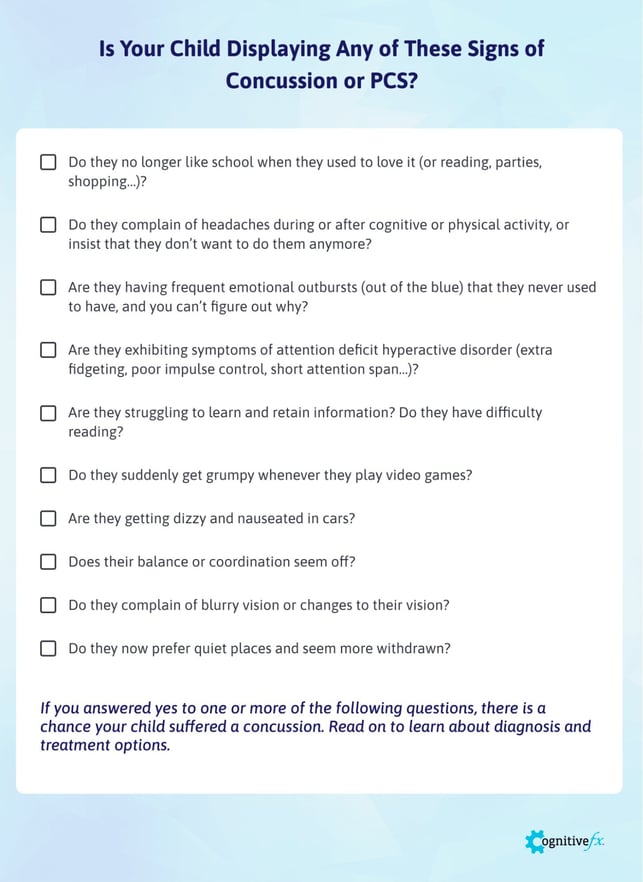
Recognizing PCS Symptoms in Children of Different Ages
One of the biggest challenges in identifying post-concussion syndrome in children is that symptoms can look very different depending on age. Children often lack the vocabulary to describe what they're experiencing, and their symptoms may manifest as behavioral changes rather than physical complaints.
Symptoms in Toddlers and Preschoolers (Ages 2-5)
Young children can't tell you they have a headache or feel dizzy. Instead, watch for:
Increased irritability, crying, or tantrums that seem out of proportion
Changes in sleep patterns (more sleep, less sleep, or difficulty falling asleep)
Loss of interest in favorite toys or activities
Regression in developmental milestones (bed-wetting after being potty trained, increased clinginess)
Changes in eating habits
Appearing dazed or "not themselves"
Balance problems or increased clumsiness
Sensitivity to light or noise (covering ears, avoiding bright rooms)
Symptoms in School-Age Children (Ages 6-12)
Elementary school children may be able to describe some symptoms but often don't recognize that what they're experiencing is abnormal. Look for:
Complaints of headaches, especially during or after school
Difficulty concentrating on homework or reading
Taking much longer than usual to complete assignments
Forgetting instructions or losing belongings more frequently
Complaints of feeling "foggy" or confused
Sudden difficulty with subjects they previously understood
Avoidance of activities they used to enjoy
Mood swings, irritability, or emotional outbursts
Complaints of dizziness, especially with movement
Nausea, particularly in cars or with screen use
Sensitivity to bright lights or loud noises
Complaints of blurry vision or tired eyes
Sleep disturbances
Fatigue that seems disproportionate to activities
Symptoms in Adolescents (Ages 13-18)
Teenagers may try to minimize symptoms to return to sports or social activities, or may not connect their symptoms to their injury. Watch for:
All symptoms listed above for school-age children, plus:
Social withdrawal or isolation
Significant changes in academic performance
Depression, anxiety, or mood changes
Memory problems (forgetting conversations, difficulty learning new information)
Difficulty with executive functions (planning, organizing, multitasking)
Feeling overwhelmed in busy environments
Problems with attention and concentration lasting throughout the school day
Personality changes noted by friends, teachers, or family
Loss of motivation
Increased screen-related symptoms (headaches or nausea while using phones or computers)
The Hidden Symptoms Parents Often Miss
A 2025 study from Children's Hospital of Philadelphia found that nearly two-thirds of pediatric concussion patients report new sleep disturbances after injury, a rate higher than previously documented. Sleep disturbance was the second strongest predictor of prolonged recovery, behind only female sex. [DOI: 10.3389/frsle.2025.1528458]
Other frequently overlooked symptoms include:
Vision problems: Double vision, difficulty tracking text while reading, trouble focusing at different distances, eye fatigue. Research shows these symptoms often persist even when other symptoms improve and require specialized vision therapy.
Exercise intolerance: Symptoms that worsen with physical activity, elevated heart rate responses to minor exertion, or a sensation that the heart is "racing" inappropriately.
Cognitive fatigue: Mental exhaustion that comes on faster than expected, difficulty sustaining attention throughout the school day, needing frequent breaks.
Emotional regulation difficulties: Crying more easily than usual, getting frustrated quickly, emotional responses that seem out of proportion to situations.
Concussion symptoms in children can be hard to pin down. Our free concussion quiz adapts its questions for children under 12, using age-appropriate symptom descriptions and severity ratings. It takes about five minutes and gives you a clear picture of where your child's symptoms stand.
Risk Factors That Make Some Children More Vulnerable
Not every child who gets a concussion develops post-concussion syndrome. Research has identified several factors that increase risk:
Pre-injury factors:
History of previous concussions (the strongest predictor)
Pre-existing mental health conditions (anxiety, depression, ADHD)
Pre-existing learning disabilities
History of migraines or headache disorders
Female sex (adolescent girls have longer recovery times on average)
History of sleep disorders
Injury factors:
Higher initial symptom severity
Loss of consciousness (though many PCS patients never lost consciousness)
Amnesia around the event
Delayed symptom onset
Post-injury factors:
Delayed return to activity (prolonged strict rest)
Return to high-risk activities too soon
Inadequate academic accommodations
High psychological stress
Poor sleep after injury
Why Girls May Face Longer Recovery Times
Research consistently shows that adolescent girls experience longer concussion recovery times than boys of the same age. A 2025 study in the Journal of Head Trauma Rehabilitation found significant sex differences in blood biomarkers related to brain injury, suggesting biological factors may contribute to these differences. [DOI: 10.1097/HTR.0000000000001110]
Several theories explain this pattern:
Hormonal influences on brain healing
Differences in neck strength and biomechanics
Higher rates of pre-existing anxiety and depression in adolescent females
Possible differences in symptom reporting
Differences in the types of sports and injury mechanisms between sexes
Regardless of the cause, girls who sustain concussions should be monitored closely and parents should be prepared for potentially longer recovery timelines.
When to Seek Help From a Specialist
Emergency Warning Signs (Seek Immediate Care)
Go to the emergency department immediately if your child experiences:
Worsening headache that doesn't improve with rest or medication
Repeated vomiting
Seizures
Weakness, numbness, or decreased coordination
Slurred speech
One pupil larger than the other
Extreme drowsiness or cannot be awakened
Increasing confusion, restlessness, or agitation
Loss of consciousness
Behavior or personality changes that are severe or worsening
Signs That Standard Care Isn't Working
Consult a specialist if your child:
Has symptoms persisting beyond four weeks
Shows minimal improvement despite following initial recommendations
Has been told to "just rest" for weeks without a clear treatment plan
Is falling significantly behind in school
Has been prescribed multiple medications without improvement
Experiences symptoms that are getting worse rather than better
Has been diagnosed with new conditions (ADHD, anxiety, depression) following the injury without evaluation for PCS
Cannot tolerate any physical activity without significant symptom flare
Has vision or balance problems that aren't improving
Finding the Right Specialist
Many pediatricians and even some neurologists don't specialize in post-concussion syndrome and may not be familiar with current evidence-based treatments. Look for:
Sports medicine physicians with concussion expertise
Neuropsychologists specializing in brain injury
Concussion clinics with multidisciplinary teams
Providers who offer functional assessment tools (not just standard imaging)
Clinics that provide active rehabilitation rather than just rest advice
What Recovery Actually Looks Like {#recovery-timeline}
The Research on Pediatric Concussion Recovery
Let's look at what the evidence actually tells us about recovery timelines:
Typical recovery (most children):
70-90% of children recover within 2-4 weeks
Median recovery time is approximately 13 days
Most improvement occurs in the first 10 days
Post-concussion syndrome (10-30% of children):
Symptoms persist beyond 4 weeks
Recovery timeline varies significantly based on treatment approach
With appropriate treatment, most children show meaningful improvement
Some children require several months of rehabilitation
Factors associated with faster recovery:
Early return to light physical activity (within 24-48 hours)
Gradual return to school (within 1-2 days)
Active rehabilitation approaches
Adequate sleep
Low psychological stress
Strong support systems
Factors associated with slower recovery:
Prolonged strict rest
Extended absence from school
Social isolation
High anxiety about symptoms
Return to contact sports before symptoms resolve
Sleep problems
What the Amsterdam Consensus Changed
The 2022 Amsterdam Consensus Statement revolutionized pediatric concussion management with several key updates:
Old approach (now outdated):
Complete rest until symptom-free
"Cocooning" in dark rooms
Avoiding all screens
Waiting for full symptom resolution before returning to school
Waiting for full symptom resolution before any physical activity
New evidence-based approach:
Brief period of relative rest (24-48 hours)
Early return to light physical activity (walking, light exercise)
Limited screen time is acceptable (complete avoidance may increase anxiety and isolation)
Return to school within 1-2 days with accommodations
Symptom-limited activity rather than complete avoidance
Active rehabilitation for symptoms persisting beyond 10-14 days
This represents a fundamental shift: prolonged rest can actually prolong recovery by deconditionining the brain and body, increasing anxiety, and disrupting the social connections children need.
Week-by-Week Recovery Expectations
Week 1 (Days 1-7):
Expect symptoms to be most severe in first 24-72 hours
Brief rest period recommended for first 24-48 hours
Light activity (walking, gentle movement) can begin within first few days
Return to school with significant accommodations
Avoid activities with high risk of another head injury
Sleep may be disrupted; maintain regular sleep schedule as much as possible
Week 2 (Days 8-14):
Most children see significant symptom improvement
Gradual increase in school participation
Light aerobic exercise if tolerated
Continue to avoid contact sports and high-risk activities
Many children return to normal by end of week 2
Weeks 3-4 (Days 15-28):
Children still symptomatic should be assessed by a specialist
Active rehabilitation may begin
Continued gradual increase in activity
Academic accommodations should be actively managed
If not improving, reevaluation of treatment approach is warranted
Beyond 4 weeks:
Consider formal PCS diagnosis
Comprehensive evaluation recommended
Targeted multidisciplinary treatment often necessary
Don't accept "wait and see" as the only strategy
The Solution: Evidence-Based Treatment Options {#treatment-options}
Why "Just Rest" Is No Longer the Answer
For decades, the standard advice for concussion was complete rest until symptoms resolved. We now know this approach is not only ineffective for many children but can actually prolong recovery.
Research shows that:
Prolonged rest leads to deconditioning
Social isolation worsens anxiety and depression
Missing school creates academic stress that compounds symptoms
Avoiding all activity doesn't give the brain the stimulation it needs to heal
The Amsterdam 2022 Consensus states clearly: "Gone are the days of complete physical and cognitive rest. 'Cocooning,' in which a patient is kept in a darkened environment with little stimulus, not only lacks benefit but may be harmful by slowing recovery."
Active Rehabilitation Approaches
Modern evidence-based treatment for pediatric PCS focuses on active rehabilitation. A 2024 study in Neuropsychological Rehabilitation found that multimodal intervention programs significantly improved symptoms in children with persistent post-concussion symptoms. [DOI: 10.1080/09602011.2024.2402564]
Aerobic Exercise Therapy
Sub-symptom threshold aerobic exercise has emerged as one of the most effective treatments for PCS. Research shows that prescribed aerobic exercise improves quality of life and reduces symptoms.
Key principles:
Exercise is prescribed at an intensity below the symptom threshold
Intensity gradually increases as tolerance improves
Typically performed daily for 20-30 minutes
Should be supervised by a trained professional initially
Vestibular Rehabilitation
For children with dizziness, balance problems, or motion sensitivity, vestibular therapy is crucial. This specialized physical therapy retrains the balance and spatial orientation systems.
A 2024 study found that adolescents who received vestibular rehabilitation showed similar benefits regardless of sex, with both males and females improving equally. [DOI: 10.1097/HTR.0000000000001113]
Vision Therapy
Given that over 60% of children with persistent symptoms have vision disorders, specialized vision assessment and therapy is often essential.
Vision therapy addresses:
Convergence insufficiency (eyes not working together)
Accommodation problems (focusing difficulties)
Eye tracking issues
Visual processing speed
Reading difficulties related to vision
Cognitive Rehabilitation
For children struggling with attention, memory, and thinking speed, cognitive therapy provides targeted exercises to rebuild these skills. This may include:
Working memory training
Attention exercises
Processing speed activities
Executive function skill building
Compensatory strategies for school
Cervical Spine Treatment
Neck dysfunction contributes to many PCS symptoms, particularly headaches and dizziness. Treatment may include:
Manual therapy
Specific strengthening exercises
Postural correction
Neuromuscular retraining
Psychological Support
The emotional impact of prolonged symptoms shouldn't be underestimated. Effective treatment often includes:
Cognitive behavioral therapy for anxiety and depression
Education about PCS and recovery expectations
Stress management techniques
Family support and education
How Cognitive FX Treats Pediatric PCS
At Cognitive FX, we take a comprehensive, multidisciplinary approach to treating children with post-concussion syndrome. Here's what makes our approach different:
Functional Brain Imaging (fNCI)
Unlike standard MRI or CT scans, which typically appear normal in PCS patients, our functional Neurocognitive Imaging (fNCI) scan shows us how different regions of your child's brain are actually functioning. This proprietary technology allows us to:
Identify which specific brain regions are affected
Measure neurovascular coupling dysfunction
Create a targeted treatment plan based on objective findings
Track improvement over time
This imaging gives parents something they often haven't had: objective proof that something is wrong and a clear path forward.
EPIC Treatment Protocol
Our Enhanced Performance in Cognition (EPIC) treatment is an intensive, one-week program designed to jumpstart recovery. The treatment follows a cycle of preparation, activation, and recovery:
Preparation: Cardiovascular exercise improves blood flow to the brain, priming it for therapy
Activation: Targeted multidisciplinary therapies challenge affected brain regions
Recovery: Structured rest periods allow the brain to consolidate gains
Therapies included may incorporate:
Aerobic conditioning
Neuromuscular therapy
Cognitive therapy
Vestibular therapy
Vision therapy
Occupational therapy
Sensorimotor integration
Psychological evaluation and support
Treatment for Children
We treat children ages 8 and up (or at a third-grade reading level). Our approach is tailored for younger patients:
Content and activities are matched to children's interests (incorporating favorite sports, games, or themes)
Therapists are trained in pediatric care and communication
Parents are involved in treatment decisions and learn techniques to continue at home
Continuous monitoring ensures children feel safe and supported
Homework assignments extend recovery beyond the clinic week
Treatment Outcomes
An independent peer-reviewed study found that 77% of patients treated at Cognitive FX showed statistically significant improvement in symptoms. Cognitive FX is the only PCS clinic with third-party validated treatment outcomes.
If your child has been struggling with post-concussion symptoms, schedule a consultation with our team. We'll review their medical history and determine if they're eligible for treatment.
School Accommodations and Return-to-Learn Protocols
Why School Matters More Than You Think
The old advice to keep children home from school until symptoms completely resolve is now considered harmful. Research shows that extended school absence:
Increases anxiety about returning
Creates academic pressure that worsens symptoms
Isolates children from social support
Delays cognitive recovery
Can lead to school refusal
The Amsterdam Consensus recommends returning to school within one to two days of injury, with appropriate accommodations. Missing school for more than a week is explicitly not recommended for most children.
The Graduated Return-to-Learn Protocol
Students should progress through these stages as tolerated, spending at least 24 hours at each stage before moving on:
Stage 1: Daily Activities at Home
Light cognitive activity at home
Reading, light screen time, conversation
Rest as needed
Stage 2: School Activities at Home
Homework assignments in short sessions
Breaks every 15-20 minutes
Limited screen time
Stage 3: Partial Return to School
Half days or shortened schedule
Maximum accommodations in place
Modified workload
Stage 4: Full Return with Accommodations
Full school days
Continued accommodations
Catching up on missed work gradually
Stage 5: Full Return Without Accommodations
Normal school participation
Full workload
Continue monitoring for setbacks
Specific Accommodations to Request
Academic accommodations for children with PCS may include:
Environmental modifications:
Preferential seating away from windows and noise
Permission to wear sunglasses or a hat indoors
Access to a quiet space for rest breaks
Reduced noise exposure (headphones during independent work)
Dimmed lighting when possible
Schedule modifications:
Shortened school days initially
Later start time if sleep is affected
Rest breaks as needed (nurse's office or quiet room)
Extended time between classes
Workload modifications:
Extended deadlines for assignments
Reduced homework load
Breaking assignments into smaller chunks
Prioritizing essential assignments
Allowing verbal rather than written responses
Reduced reading requirements
Testing modifications:
Extended time on tests and quizzes
Testing in a quiet environment
Frequent breaks during testing
Oral testing options
Reduced test length or separate sessions
Support services:
Access to notes from teachers or peers
Audio recordings of lectures
Tutoring support for missed content
Check-ins with school counselor or nurse
504 Plans vs. IEPs
504 Plan: Provides accommodations within regular education. Appropriate for most students with PCS. Faster to implement and modify.
IEP (Individualized Education Program): Provides specialized instruction and related services. May be needed if PCS causes significant, long-term educational impact.
Most children with PCS will benefit from a 504 plan. Work with your school's 504 coordinator to develop appropriate accommodations.
Sample 504 Plan Language
When requesting accommodations, specific language helps. Examples:
"Due to post-concussion syndrome, [Child's Name] requires extended time (time and a half) on all tests and quizzes, to be administered in a quiet environment separate from the classroom."
"[Child's Name] is permitted to take rest breaks as needed, signaled to the teacher by [agreed-upon signal], with access to the nurse's office or other quiet space for breaks lasting 10-15 minutes."
"Homework assignments will be reduced by 50% during the accommodation period, with priority given to core concepts as identified by the teacher."
Communicating with Teachers
Effective communication with your child's teachers is essential. Consider:
Requesting a team meeting with all teachers at once
Providing written documentation from your child's healthcare provider
Sharing specific accommodation requests
Establishing a communication system for reporting symptom flares
Scheduling regular check-ins to adjust accommodations
Remember: teachers want to help but may not understand concussion. Brief education about PCS can go a long way.
Return-to-Play Guidelines for Young Athletes
The Six-Step Graduated Protocol
Following the Amsterdam 2022 guidelines, young athletes should complete this graduated return-to-play protocol after being cleared for activity by a healthcare provider. Each step should take at least 24 hours, with return to the previous step if symptoms worsen.
Step 1: Symptom-Limited Activity
Light walking, swimming, stationary cycling
Intensity: light enough to hold a conversation
Goal: Reintroduce movement without symptom exacerbation
Step 2: Light Aerobic Exercise
Walking, swimming, or cycling at moderate intensity
No resistance training
Goal: Increase heart rate
Step 3: Sport-Specific Exercise
Running drills, skating drills (no head impact activities)
No contact or activities with risk of head injury
Goal: Add movement patterns
Step 4: Non-Contact Training Drills
Complex drills, resistance training begins
May begin practice with team (non-contact)
Goal: Exercise, coordination, cognitive load
Step 5: Full-Contact Practice
Normal training activities after medical clearance
Must complete step 5 (full-contact practice) before competition
Medical clearance required before steps 5 and 6
Children under 18 should not return to competition on the same day as the injury
What the 2022 Updates Changed
The Amsterdam 2022 Consensus made several important updates to return-to-play protocols:
Previous guidance: Complete rest until symptom-free, then begin graduated protocol.
Current guidance: Brief rest (24-48 hours), then begin symptom-limited physical activity. The graduated protocol now begins earlier, with light activity permitted even while mild symptoms persist.
Why this matters: Emerging evidence shows that early, controlled physical activity may actually promote recovery rather than delay it. Athletes who remain completely sedentary may decondition and experience prolonged symptoms.
Reducing Future Concussion Risk
Once your child returns to sports, consider these evidence-based prevention strategies:
Proper helmet fitting (though helmets don't prevent concussion, they reduce severe injuries)
Mouthguard use (associated with lower concussion rates in some studies)
Rule enforcement (body-checking restrictions in youth hockey significantly reduce concussions)
Neuromuscular training programs
Appropriate supervision and coaching
Honest reporting culture (athletes should feel safe reporting symptoms)
What You Can Do at Home to Support Recovery
Daily Strategies for Parents
Sleep optimization:
Maintain consistent sleep and wake times
Limit screen use before bed
Create a cool, dark sleeping environment
Address any new sleep problems with your healthcare provider
Activity pacing:
Help your child identify their symptom threshold
Break activities into manageable chunks
Schedule rest breaks proactively
Monitor symptoms during activities
Screen time management:
Limit recreational screen use while symptomatic
Use screen settings that reduce brightness and blue light
Take frequent breaks (20-20-20 rule: every 20 minutes, look at something 20 feet away for 20 seconds)
Note: Complete screen avoidance is no longer recommended
Encourage daily light physical activity as tolerated
Walking is excellent for recovery
Avoid activities with risk of head injury
Balance exercises can help vestibular recovery
Cognitive Exercises at Home
Once your healthcare provider approves, gentle cognitive activities can support recovery:
Word games and puzzles (start simple, progress gradually)
Memory games (matching cards, recall exercises)
Reading (short sessions with breaks)
Simple board games
Light conversation and social interaction
Key principles:
Stop if symptoms significantly worsen
Short sessions (10-15 minutes) with breaks
Gradually increase difficulty and duration
Make it enjoyable, not stressful
Emotional Support Strategies
Post-concussion syndrome takes an emotional toll on children and families. Support strategies include:
Validation: Acknowledge that symptoms are real and frustrating. Avoid phrases like "it's all in your head" or "just try harder."
Patience: Recovery can be slow. Celebrate small improvements rather than focusing on remaining limitations.
Hope: Remind your child that most children with PCS do get better with appropriate treatment.
Connection: Maintain social connections when possible, even if activities need to be modified.
Professional support: Don't hesitate to involve a mental health professional if anxiety, depression, or mood changes become significant.
When to Worry About Worsening Symptoms
Contact your healthcare provider if:
Symptoms significantly worsen rather than gradually improve
New symptoms develop
Your child's functioning declines notably
Symptoms that had improved suddenly return
You're concerned about depression, anxiety, or mood changes
Medications seem to be making things worse
Frequently Asked Questions {#faq}
How long does post-concussion syndrome last in children?
Most children recover from concussion within two to four weeks. Post-concussion syndrome is diagnosed when symptoms persist beyond four weeks. With appropriate treatment, most children with PCS show significant improvement within one to three months. Some children may require longer treatment periods, particularly if they have risk factors like previous concussions or pre-existing conditions.
Can PCS cause permanent damage?
Post-concussion syndrome does not typically cause permanent brain damage. The brain has remarkable capacity for healing, particularly in children. However, prolonged symptoms that go untreated can lead to secondary problems like depression, anxiety, academic difficulties, and social challenges. This is why early, appropriate treatment is important.
How can I tell if my child's symptoms are from PCS or something else?
This is where professional evaluation becomes crucial. Symptoms of PCS can overlap with anxiety, depression, ADHD, learning disabilities, and other conditions. A comprehensive evaluation by a specialist can distinguish between these possibilities. Sometimes multiple conditions exist together and all need to be addressed.
Should my child see a neurologist?
A pediatric neurologist can be helpful in some cases, particularly to rule out other neurological conditions. However, many neurologists don't specialize in post-concussion syndrome and may not offer the multidisciplinary treatment most children need. Look for providers specifically experienced in PCS treatment rather than assuming any neurologist will be the right fit.
Is it safe for my child to use screens?
Current evidence does not support complete screen avoidance after concussion. Moderate screen use is generally acceptable, though some children may need to limit screens that worsen their symptoms. Pay attention to your child's individual response and adjust accordingly. Complete isolation from screens may increase anxiety and social isolation without providing benefit.
When can my child return to sports?
Children should complete a graduated return-to-play protocol and receive medical clearance before returning to contact sports. This process takes a minimum of one week after symptoms resolve but often takes longer. Never return a child to contact sports on the same day as a concussion, regardless of how minor it seems.
What if my doctor says to "just wait it out"?
If your child has had symptoms for more than four weeks without improvement, "waiting" is not a treatment plan. Seek evaluation from a specialist with expertise in post-concussion syndrome. Active rehabilitation, not passive waiting, is now the evidence-based standard of care.
Are medications helpful for PCS?
Medications may help manage specific symptoms but don't treat the underlying dysfunction. Be cautious about:
ADHD medications combined with sleep medications (creates a problematic cycle)
Overuse of pain medications (can cause rebound headaches)
SSRIs in children (require careful monitoring)
Discuss any medications carefully with a provider familiar with pediatric PCS.
How do I know if treatment is working?
Signs of improvement may include:
Reduced symptom severity
Longer periods without symptoms
Improved tolerance for activities
Better school performance
Improved mood and energy
Better sleep quality
Return to activities previously avoided
What if we can't afford specialized treatment?
Some options to explore:
Insurance coverage (many treatments are covered)
School-based services (therapy through the school system)
Outpatient rehabilitation programs
Home exercise programs prescribed by a physical therapist
Community-based support groups
Even if intensive treatment isn't immediately accessible, working with your primary care provider to implement active rehabilitation principles can help.
Taking the Next Step
If your child has been struggling with symptoms following a concussion, you don't have to accept that this is just how things will be. Post-concussion syndrome is real, it's treatable, and most children can make meaningful recovery with the right approach.
The first step is getting proper evaluation from providers who understand PCS. Whether that's at Cognitive FX or another specialized clinic, the key is finding healthcare providers who offer:
Comprehensive assessment beyond standard imaging
Active rehabilitation rather than just rest advice
Multidisciplinary treatment addressing all affected systems
Clear communication and measurable goals
Ready to get answers about your child's symptoms?
Schedule a free consultation with the Cognitive FX team. We'll review your child's medical history and determine if they're eligible for treatment at our clinic.
95% of our patients show statistically verified restoration of brain function after treatment. Your child deserves to feel like themselves again.
{{cta('124586502405')}}
References and citations are available upon request. This article incorporates current research from PubMed and guidelines from the 2022 Amsterdam Consensus Statement on Concussion in Sport.
Dr. Alina Fong, PhD, is a Clinical Neuropsychologist and co-founder of Cognitive FX. She holds a doctorate in Clinical Neuropsychology and has dedicated her career to developing evidence-based treatment protocols for brain injury patients.
Dr. Lynn Gaufin graduated from the University of Utah and then attended medical school at Cornell University in New York City. After medical school he join the Army and was a surgeon in the military before finishing his Neurological Residency at University of California Los Angeles. Dr. Gaufin specializes in cervical and lumbar spine surgery, brain tumors, brain hemorrhages, and treatment of traumatic brain injuries. Dr. Gaufin is one of the emergency trauma neurosurgeons on call at Utah Valley Hospital. Before he began his practice in Utah he saw a significant amount of traumatic brain injuries during his career in the Army and his residency in Los Angeles. As a surgeon who treats individuals who suffer from mild to severe traumatic brain injuries he recognized a problem in the post operative rehabilitation. Individuals who suffered severe trauma would be admitted into speciality facilities where they would receive months of care. But patients who had a more mild trauma would be released and would largely be on their own when it came to restoring their cognitive function. That problem is what lead Dr. Gaufin to team up with Dr. Fong and Dr. Allen in the creation of Cognitive FX. Cognitive FX was able to take the research that Dr. Fong and Dr. Allen started in their Phd programs and bring it into the clinical environment.
Related Posts
Can Lyme Disease Cause Memory Loss, and Is It Reversible?
If you've searched "is Lyme brain fog permanent" or "will I ever think clearly again," you're not alone. And more importantly, you deserve a real answer based on actual science, not empty...
Deep TMS delivers magnetic pulses through a coil shaped like the letter H, held inside a cushioned helmet. The H-coil's magnetic field drops off more...
Dysautonomia is an umbrella term for disorders in which the autonomic nervous system, the network that automatically runs heart rate, blood pressure, digestion, and temperature, stops regulating the...
Published peer-reviewed research shows that Cognitive FX treatment leads to meaningful symptom reduction in post-concussion symptoms for 77% of study participants. Cognitive FX is the only PCS clinic with third-party validated treatment outcomes.